
So we had a pretty interesting patient last week that you'll read about in a hot second. The PT chose one exercise that ended up with amazing results. We thought we share about this patient's plan of care, describe the awesome corrective exercise used to improve squat mechanics (and apparently abolish anterior knee pain).
Case Report:
Subjective: Patient is a 49 y.o. male with a chief complaint of bilateral knee pain and weakness.
Onset: 3mo ago prolonged driving
Worse: knee flexion and squatting
Better: extending/stretching knees.
Pain: constant, ranging from 4-8 out of 10 depending on activity level. Location was bilateral anterior knee pain superior to patella.
Objective evaluation showed knee strength and ROM within normal limits and pain free. Pt was point tender with palpation to bilateral superior border of patella. SFMA was performed to further screen movement and he was found to have dysfunctional and painful Overhead squat (OHS) and a dysfunctional and non-painful Multi-Segmental extension (MSE). OHS was dysfunctional due to excessive anterior motion with knees, minimal to no posterior motion with pelvis, knee valgus, lack of squat depth, heel rise and loss of UE height. MSE was dysfunctional due to aberrant motion and lack of anterior hip motion, and high RPE. Upon further breakout of the OHS, the patient was found to have a stability/motor control deficit (SMCD) for his overhead squat pattern as he in fact had all of the mobility necessary to complete the motion of the overhead squat when each joint was checked individually.
Treatment for the SMCD included RNT (Reactive Neuro-muscular Therapy) Overhead Squat 2x15 to promote posterior hip movement with cues for patient to squat without lifting heel. Pain was abolished halfway through second set of RNT. Pt was able to perform OH squat without assistance and was issued for home program 15 times every 2-3 hours. Upon return to therapy the patient showed functional and non-painful patterns for OHS and MSE.
I found it interesting that the dysfunctional compensations were the opposite for each of the two dysfunctional patterns as OHS actually needs posterior pelvis movement and MSE actually needs anterior pelvis movement to be performed properly. I hypothesize that these two motions are more closely related than we think in regards to motor control. He presents in the clinic as if the two wires are crossed for these fundamental motions as the compensations are opposite. This is a great example of how functional movement carries over from one functional exercise to another as an improvement on one can correct deviations from the norm in other patterns. The RNT drill had not only corrected all compensations with the OHS but also corrected all compensations for the MSE. I guess you can say he was essentially re-wired.
Corrective Exercise: RNT Overhead Squat
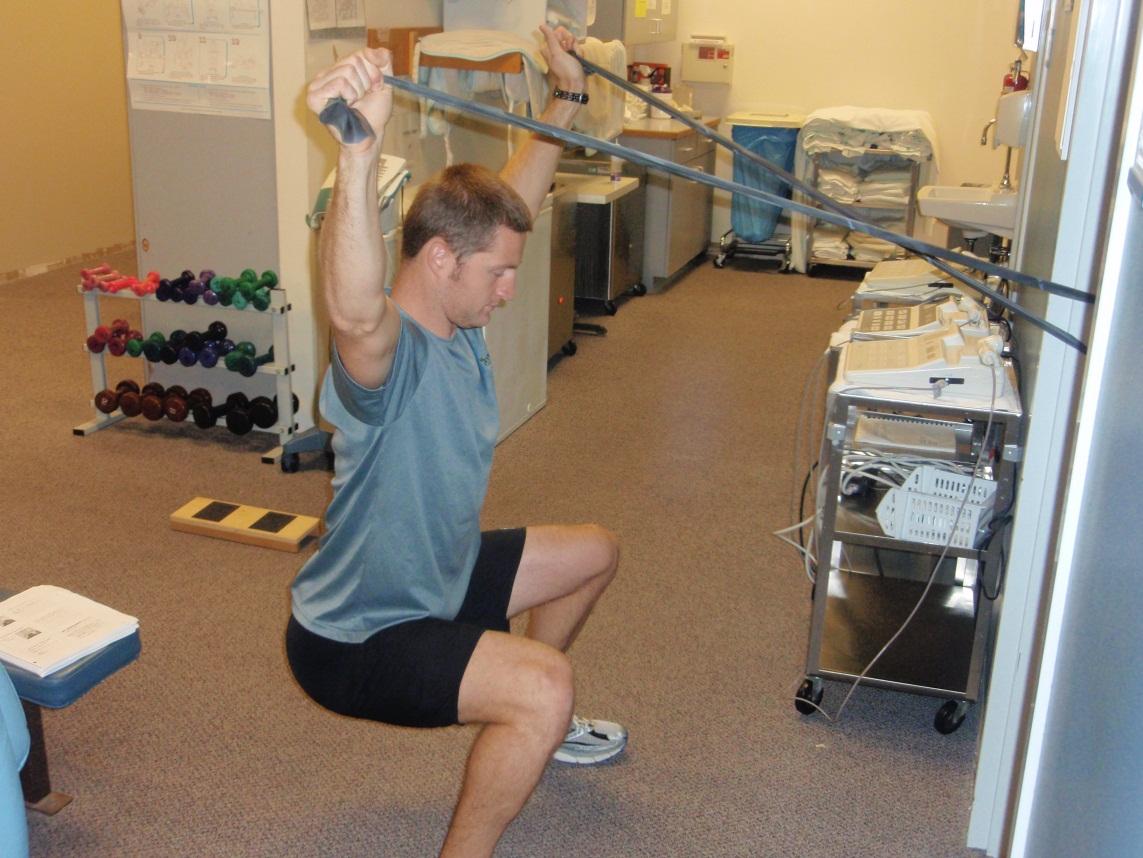
Why it works:As you read above the patient had multiple compensatory strategies, especially at the hip and trunk. After faulty movements are performed over time, the body does not realize its moving poorly. This allows the body to change tension and recruitment of muscles in the hip as well as change its overall body awareness (proprioception) of the hip and pelvic joint. Left unchecked, these changes likely lead to the patient's knee pain.
So RNT essentially gives the muscle, and more importantly the brain and nervous system, the ability to notice its faulty movements by feeding into the dysfunction. This gives the body the ability to self-correct. Instead of telling someone not to do something, you retrain the movement by pushing into the wrong movement thereby allowing a reaction to facilitate the neuromuscular system to correct and thereby produce a better muscular recruitment pattern. Specifically, for this exercise, the bands are pulling the patient forward causing a reaction to pull back (with the arms as well as the hips) to keep the trunk upright. This activates the core and provides a posterior pelvic tilt moment, allowing for less tension in the hips that will pull you forward. This also cues the body to sit back,rather than shift forward, because it throws the patient forward if they don't resist. How do I use it: I think its best as a dynamic warm up before any squats, cleans, snatches,etc. Test your squat intermittently through the day and if your shooting forward or closing up than knock out 5-10 reps, just hook it to a door knob and rock them out, longer carryover is all about early compliance and consistency!