
Patients get so wrapped up in what their doctor said of their MRI impression. In addition, chances are that poor education followed. Stating things like “torn” or herniated” don’t necessarily build confidence of any type in the patent.

In fact, MRI findings will increase the fear of their condition, which in turn increases their awareness of their pain... “The use of degenerative terms such as wear and tear by patients is associated with a poor perceived prognosis.” We can do better...and better education will make the patient more invested in their treatment and more compliant with their plan of care.
So when your patient argues: “I hear what you're saying about making me move better so I can feel better, but I have a torn this or a herniated that.” (note the defeat in their tone).
Here are 7 rebuttals on why you shouldn't’ put so much stock, and more importantly let your patients put any stock into their imaging.
- “So I am hearing that you have a herniated disk and/or stenosis. Is your pain constantly the same in all positions and movements? NO...then where did your stenosis(fill in the blank) go? If the lesion is constant but your pain isn’t then it's unlikely that whichever pathoanatomical condition that was seen by imaging is the source of all of your pain. (I may agree that it can be playing a part). Further, there’s likely positions and movements that your body will like. If we can find these then you have a really good chance of having positive outcomes for relief and return to function!
- “Are you more concerned about your herniated disk or your pain and its effects on your day to day life? Let me help you better understand your pain which can go a long way towards you actually feeling and moving better” (For chronic musculoskeletal pain disorders, there is compelling evidence that an educational strategy addressing neurophysiology and neurobiology of pain can have a positive effect on pain, disability, catastrophization, and physical performance). We won't go into pain science on this. Mosley, Butler, and Louw do an amazing job teaching this concept.
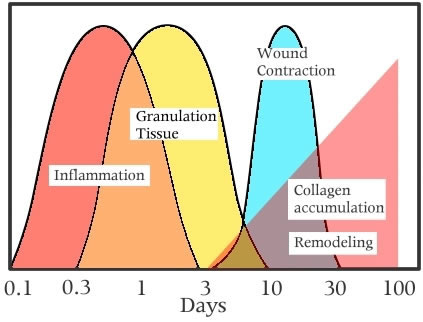
- “band aid/ tissues heal analogy”: How long ago did you start feeling pain, over 3 months? Lets say you had a bad cut on your leg at the same time. You put a band aid on it and for the most part took care of it. Would you cut still be bothering you? Of course not. Your tissue, for all extensive purposes, has completely healed! This is the same for your injury; tissues heal! Your inured tissues goes through inflammation and repair themselves like any other injury. Of course you have maybe a tiny scar left over from your cut and you may have little deficits noticed on the MRI, but again, your tissue that requires you to move and hold postures has healed! Your pain, and your impression on the MRI, is not completely a consequence of injured tissue.
- Was your MRI performed supine on your back? Do you live on your back? Of course not, so its not the best representation (insert validity) of what your back looks like while you're standing and moving. In fact, research demonstrates that disc look different between static and dynamic (movement) MRIs!
Further, while laying in supine gravity is pulling your disc down, possibly making your disc look worse than it is, and giving you a unrealistic look at your spine.
- When was your MRI completed? In the morning? Well gues what, you discs change height during the day and even get reabsorbed back in. Typically a morning MRI will be less realistic of what's going on.
- 40% of people with NO Back pain have a bulging disc. Look around this clinic, about half of us PTs likely have some lesion/deficit in our back that is NOT bothering us.
- Finally, discs go back into place, sometimes completely on their own. Therapy has been shown to be a very effective way to improve proper disc alignment into their normal resting position.
I know what we all learned in school: “MRIs are the gold standard” but they come with an inherent risk. Risks that jeopardize the overall outcomes and success of medical practitioners.
Just like how medicine has side effects, those ordering MRIs need to analysis and consider the side effects that come with ordering MRIs:
- “If you want an excuse to operate on a pitcher’s throwing shoulder, just get an M.R.I.,”Dr. Andrews says
- Dr. Sangeorzan said. “It is a very sensitive tool, but it is not very specific. That’s the problem.” And scans almost always find something abnormal, although most abnormalities are of no consequence. Please read more on the overuse of MRIs in this NY times article.