
The Infraspinatus might be one of the most problematic muscles in the upper quarter in my experience. This makes sense due to the constant stresses we put on it with our posture and repetitive stresses. Our forward, rounded shoulders and repetitive forward lifting will result in altered scapular positioning; specifically anterior tilted and internally rotated. There is a growing body of literature associating abnormal shoulder kinematics and with a variety of shoulder pathologies. In fact “evidence for scapular kinematic alterations in patients with impingement or rotator cuff symptoms is substantial” according to Ludewig and Reynold’s study The Association of Scapular Kinematics and Glenohumeral Joint Pathologies. In it they found 9 of the 11 studies identifying alteration in scapular kinematics and its effects on issues like frozen shoulder and shoulder impingement.
These abnormal scapular postures puts an increase load on the infraspinatus. Specifically it adds an additional tension by taking the insertion on the greater tubercle of the humerus and rolling it forward. Further strain is put on this muscle with the increase load of being tilted forward thereby increasing its moment arm, and thereby torque, with any shoulder motion.


(notice how the shoulder blade can roll and tilt forward with poor posture)
This constant loading makes the muscle prone to trigger points. Trigger points (TrP) develop in this muscle over time because of the Henneman's size principle. Because the muscle is under constant load and stress ACh is constantly being released to the slow twitch fibers in the infraspinatus. ACh release leads to the muscle contracting, however due to constant firing the muscle will fatigue otu and stay locked up due to the lack of Oxygen and instabiliry to relax. This ‘energy crisis’ is due to the increased energy consumption of the muscle to stay tuat and inability to receive supplies due to ischemia from the constant contraction. Here’s a simple picture to review:

In fact, infraspinatus TrP are very common according to research. Bron et al, in their research ‘High prevalence of shoulder girdle muscles with myofascial trigger points in patients with shoulder pain’ found the infraspinatus to be the most common active TrP in the shoulder girdle. Infraspinatus TrP are common in everyone, whether postural from computer work (white collar) or repetitive manual labor (blue collar). An article from the Clinical Journal of Pain stated “Blue-collar and white-collar workers exhibited a similar number of TrPs in the upper quadrant musculature. The referred pain elicited by active TrPs reproduced the overall pain pattern. The distribution of TrPs was not significantly different between groups”, finding the Infraspinatus again the most prevalent involved muscles.
Now that the importance of relieving the infraspinatus has been noted, I want to list a few ways to rule in infraspinatus pathology.
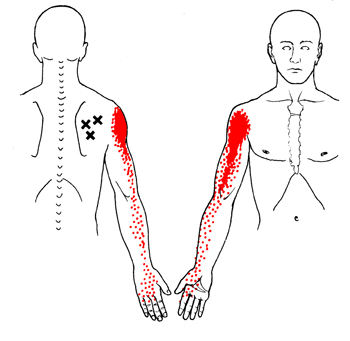
1. pain referral in shoulder/AC and radiating into delt and upper arm (and possibly lower); usually stays on lateral side. Further, pain is reproduced with palpation at the infraspinatus or allodynia (painful response to a non-painful stimulus; ie pain with a low threshold touch) is present, usually at the superior medial infraspinatus near the spine of scapula.
2. onset: symptoms develop from overuse overhead or lifting or from computer work
3. pain and weakness with resistive ER that may reproduce some or all of the patient’s pain
4. Asymmetry with IR/ADD scratch test. Additionally use this as a pre and post test assessment
5. superior humeral glide noted at or above 90degr. Due to how important the infraspinatus stabilizes the humeral head down.
When all or multiple clinical manifestations above are present than focus for the intervention should be on infraspinatus “release”. I perform the following:
1. test motion: either OH elevation or IR scratch
2. TrP DN infraspinatus, assuring a LTR is facilitated and then released.
3. IR contract relax stretching at neutral/extension, at 30 degrees and 60 degrees elevation to maximize infraspinatus tissue extensibility as noted in this cadaver study.
4. retest motion
5. IR MWM to facilitate the new tension and mobility
6. scapular diagonals with resistance and PNF lift/chop to facilitate normal movement patterns and start retraining the infraspinatus in functional patterns.
Decreasing TrP in the infraspinatus may infact decrease active and latent TrP in other muscles. Fixing the key player and other muscles will get in line. Thats why great teams always have great leadership. But don't take my word for it, research from american journal of physcial rehab and medicine concluded “that dry needle-evoked inactivation of a primary (key) MTrP inhibits the activity in satellite MTrPs situated in its zone of pain referral”.