
The Levator Scapulae (LS) is a very problematic muscle and is associated with tension type Headaches, shoulder impingement, and neck pain and stiffness, just to name a few. LS TrP can easily cause motor control issues with the kinematics if shoulder and neck motion, because of the constant loading on it. Its a muscle that's very active with all regular shoulder and neck motions because of its attachment on the shoulder blade and cervical vertebrae. Janda stated that all movements of the arm, regardless of speed or resistance requires at least some LS activation.
Because this muscle is so active it can easily become overused especially when you add on the constant tension that's put on it with forward, rounded shoulder. The overuse and postural stresses on the muscle can lead to overfaciliation during motions like shoulder overhead elevation causing the shoulder to shrug up and than the humerus to get stuck against the acromion. Usually the upper trap (UT) gets blamed for this where in reality it's the LS that is elevating the shoulder and preventing normal upward rotation of the scapula and disengaging the serratus, middle and upper trap. Here are a few things to examine to Rule in LS deficits:
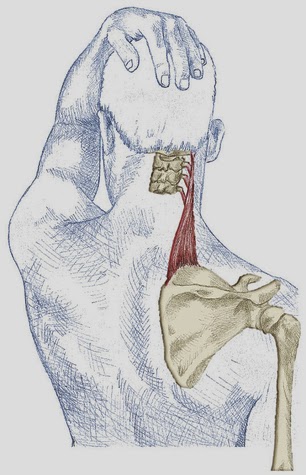
LevatorScapulae Clinical Prediction Rule:
1. TrP Assessment: low pain threshold with palpation and pain referral as noted below. This pain referral is classic and can easily get blamed by the UT or rhomboids. However UT will be more lateral pain and go near the temporal region, it also doesn't go into the periscap region typically. I start with rolling off the medial border of the spine of scapula and working superiorly and medially perpendicular to the muscles belly. Taut bands and twitching can be found noticeably even though the muscle is under the middle trap (MT). BE sure to palpate perpendicular to the LS and not the MT. The LS can also be palpated better with the pt going into a hammer locked position (IR scratch position).


2. movement assessment: A: asymmetry &/or pain with neck flexion/rotation/SB coupled motion, specifically more loss or pain with this contralaterally. So if your thinking R LS issues than L flex/rot motion will be more limited. I have the patient try to reach their chin to touch mid clavicle with my finger as an external cue. Pay attention to quantity and quality of motion. Also pain may be reproduced with ipsilateral cervical rotation or this coupled motion during motion or at end range.

B. Asymmetry with supine passive end range neck rotation with scapula depression; specifically contralateral loss. This allows you to isolate the LS because its the only muscle that is stretched with contralateral rotation and passive scap depression. This additional test was suggested inThe Journal of Manual and Manipulative Therapy and had more positive findings of LS tightness. TrP will lead to stiffness and asymmetry in this motion further improving your clinical decision.
If "1" and "2" are both occurring than the LS is problematic and at the least leading, if not causing, their impairment. Applying a "TrP assessment" with a "Movement Assessment" helps differentiate between other posterior cervical soft tissue including the UT and splenius cervicus.