
Lets talk about your heel pain or the patient just referred with a Dx of plantar fasciitis. 
First off, a majority of plantar fasciitis are incorrectly diagnosed. I would say a majority of those Dx with plantar fasciitis do not have actual plantar fascia/aponeurosis issues, in regards to tissue morphology. Thats because the super strong fascia band, similar to a piece of steel, is slamming the supple, soft foot intrinsic muscles into the another super dense structure; bones. this makes the intrinsics the limiting factor for injury. Add on top of that the repetitive eccentric motion of the intrinsic, the most likely cause of TrPs, and you have a recipe for disaster. Yet we so often miss this because we push on the TrP and the plantar fascia and assume its the later.
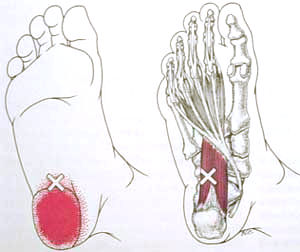
Look how similar the pain location can be below. In addition, TrP in the intrinsics can also have similar manifestations in pain like morning stiffness and history of increases in recent activity as well as weight/body mass.

In the october issue of JOSPT a group of podiatrist tried to look at the morphology of the plantar fascia with ultrasound doppler. The rationale being that “localized hyperemia (increased blood flow) is an established feature of tendinopathy, suggesting that neurovascular in-growth may contribute to tendon-associated pain in some patients. The presence of abnormal soft tissue vascularity can be assessed (and thereby confirme plantar fasciitis) with Doppler ultrasound, and assist with targeted treatment plans”. Sounds like a great idea. However, hyperemia of the plantar fascia was present in 8 of 30 participants with plantar fasciitis and in 2 of 30 controls , and only 3 were found to have moderate or marked hyperemia. So only 10% of the patients with plantar pain had actual plantar fascial issues according to the research. Their conclusion was “Mild hyperemia can occur with plantar fasciitis, but most individuals will not exhibit greater soft tissue vascularity when assessed with routine Doppler ultrasound”. But I feel they missed a huge point: if we know that hyperemia is part of the pathology and no hyperemia is involved, then it must not be the plantar fascia! There’s limitations like if the ultrasound doppler is sensitive enough for example, but this does demonstrate the importance of looking at other soft tissue structures.
Unfortunately, we also go about treating soft tissue in the plantar foot all wrong by smashing them (ALONG WITH THE PLANTAR FASCIA) with lacrosse balls and the likes. If that was helpful then excessive pounding from activities like running and box jumps would be beneficial, which we know are not. We need to be able to get to the muscles (and get our twitch response) to relief the TrP without putting pressure on them that lead to the issue in the first place.
Insert the powers of Trigger Point Dry Needling (TDN):
 |
Look for a depression between the navicular and distal medial calcaneus.
|
With TDN, like shown above, we can ‘reset’ the muscle to its normal length, improve blood flow, and improve the neuro-physiological effects by relaxing the neural input that kept the muscle locked up (as a protective response). In fact, TDN for heel pain has been shown to be effective in pain reduction in a randomized control trial this year.
Following TDN we can integrate this muscle to maintain its relieved tension by stretching, typically most effective in a loaded position. I like to use the prostretch.

Then we can retrain with eccentric loading like Single Leg Deadlifts and eccentric heel raises and reinforce with education of proper energy conservation, shoe wear, and with a heel cup taping.
With the addition of TDN, most patients can find ~100% relief in a matter of 1-3 appointments from my experience! So if you're having that nagging heel pain that won't go away try the above combination or contact us for an appointment. and receive treatment from a certified specialist.