Pain is a protective strategy to a mechanical or chemical deficit. In short, pain is only a RESPONSE. Just like my stomach grumbling is a response to hunger or
delayed onset muscle soreness in my quads is a response from a long bike ride or goose bumps are a response to being too cold...you get the point. Our body has several natural mechanisms built in to respond to the environment and stresses put on it. Pain is just one of those response systems. And they are all well needed symptoms. Imagine if your body didn't tell you, via goosebumps (piloerection), that you were too cold. Think about the potential consequences like hypothermia. In short, you would fall out of equilibrium.
 |
pain is just like goosebumps. responding to the environmental stresses
|
Consider even the consequences of not having pain. My first thought goes to the amputees I've treated. Why did they lose their foot? An infection that spread from initially stepping onto a rusty nail. A foot they did not perceive the pain of the nail. And therefore an inability to respond to the nail... I'm sure they would all be more than happy to have their pain response back.
So if pain is a neural response it begs the question what is it a response to? Often pain is a response to excessive mechanical stresses (be it overuse, compensation, postural, or traumatic) put on any number of soft tissue structures that exceed the mechanical threshold of those structures. Heres a simply analogy:
Essentially, the brain is being the protective big brother so the wimpy little brother (ie over worked soft tissue,etc) doesn’t get hurt any further or prevents it from even getting hurt. You keep picking on the little brother (with poor form or postural stresses) and the big brother will let you know (with pain). Continue to pick on the little brother and the big brother will make itself more and more known to make sure you back off. This is known as sensitization. This includes:
1. Increases in spontaneous activity secondary to increase synaptic efficiency. ie: easier to turn on pain
2. Lower threshold for pain. (hyperalgesia) Mense et al demonstrated increased/amplification of response will change so that low threshold input is necessary to turn on pain.
3. Increase response to normal stimulation (allodynia). ie: Recruitment of subthreshold inputs.

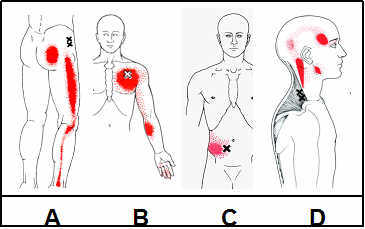
4. Enlargement of receptive field (other levels at dorsal horn)/ referred pain (secondary hyperalgesia). This explains the large referral pattern of several muscles and other soft tissue structures.
Sensitization is a continued response to pain, and therefore a continued response to movement dysfunction. We find out who is picking on the little brother we can get the big brother to back off.
Therefore, lets take pain and correlate it to movement dysfunction and a possible corresponding movement preference. Here’s a great line from Gray Cook:
“The two things I want from the patients who come into my clinic are what they tell me and what they don’t tell me. That’s why I’m such a big proponent of doing movement tests. If I make you feel better but move worse, I don’t pat myself on the back. I need to make you move better.
Sometimes you’ll temporarily feel worse, but the next day, you’ll feel much better. That’s fine, but I have to be able to change movement with what I do in order to feel confident we’re moving in the right direction. I’m not just doing this to make you temporarily feel better. I have to change movement.”
As a PT I can’t claim to be a pain specialist. I can hope to be a movement specialist. Luckily, thats enough. Luckily the body will respond by abolishing pain when we get movement better (not perfect, just better!). Back to the previous analogy, we just have to stop picking on the little brother.
Movement allows us to find out what exactly is annoying the big brother.