
So nothing like waking up to a perfect fall day and headed to a window-less classroom for the entire day. Luckily, with really good material and a great instructor the day seemed to move fairly fast. Here are some highlights, or ‘knowledge nuggets’ is you will, from day 2 of MDT for the cervical spine (and actually the end of day 1).
- when assessing the during and after response to repetitive movement, I would say the after is more important for clinical decision making. So, be slightly less concerned about the pain during the repetitive testing & more concerned about how it effects the symptoms after
- red light: worse, peripheralisation
- yellow light: NW (increase the force), NB
- green light: better, centralization
- if you're sure its a derangement. just stick with the force when you abolish/centralized it. don't try to increase it too quickly. you have the adequate amount of force/overpressure needed.
- i know i want to try to progress it in force too quickly...
- overpressure can tell us 3 things:
- reduces derangement
- exposes dysfunction, will not become variable
- exposes lateral component, exhausted sagittal plane
- when do you progress the force?
- decr or abolished during, NB after or
- prod, NW
- NE
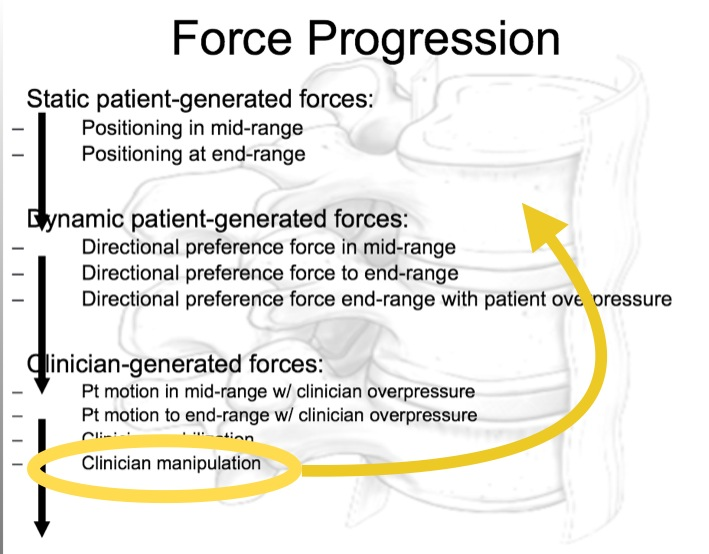
- the sequence and progression of force starts at midrange (posture correction) then end range then endrange + OP
- i love analogies, heres a good one: the “flossing your gums” analogy:
- it hurts if you haven’t flossed in a while and it will be sore after but its good for you and will make you feel better after.
- again the things that are good for them and the things that make them feel better are usually two different things initially.
- regardless of classification. ALL need posture correction/education
- shrug to get more lateral flexion to ensure end range. this is similar to pattern assist for neck reloading for SFMA people
- if its NE with upright, fixed sitting posture compared to slouched posture in sitting then start thinking possible lateral component
- C/S SB is a force progression compared to rotation
- great ergonomic videos for your patients:
- 70-75% chance respond to extension with radicular symptoms above or to the elbow
- later shifts has a relevant lat components. not all relevant lat components have a lateral shift
- below the elbow radicular symptoms may have a higher likelihood of having a relevant lateral component
- what do we observe during movement loss?
- quality such as uniform curve and curve reserval
- deviations (lateral)
- quantity
- symmetry
- when in doubt/ they are “mechanically inconclusive”. FLEX them/provocate them because this gives you more information. And educate them on why you're doing this.
- self-Rx for dysfunction every 2-3hrs, 10-15 rep into provocative position
- differentiate derangement from a adherent nerve root with RFIL